MEMPHIS, Tenn. — As Thanksgiving approaches, many people have considered rushing to get a rapid COVID-19 test that would offer a result which could mean spending time with extended family.
However, WREG has learned a negative test result doesn’t mean a person isn’t infected with COVID-19. It’s one of the reasons some have raised questions about the tests, including their use on at-risk seniors.
Manufacturers describe the rapid COVID-19 tests sent to nursing homes across the country and here in the Mid-South as fast, reliable and easy to use. They produce “on-the-spot” results, in some cases in only 15 minutes, allowing nursing homes to avoid having to wait on results from a lab.
The Centers for Medicare and Medicaid Services distributed rapid, point-of-care testing kits to 13,850 to nursing homes nationwide.

CMS distributed the point of care testing kits in three waves in the summer and fall, starting with hot spots, which included Shelby County.
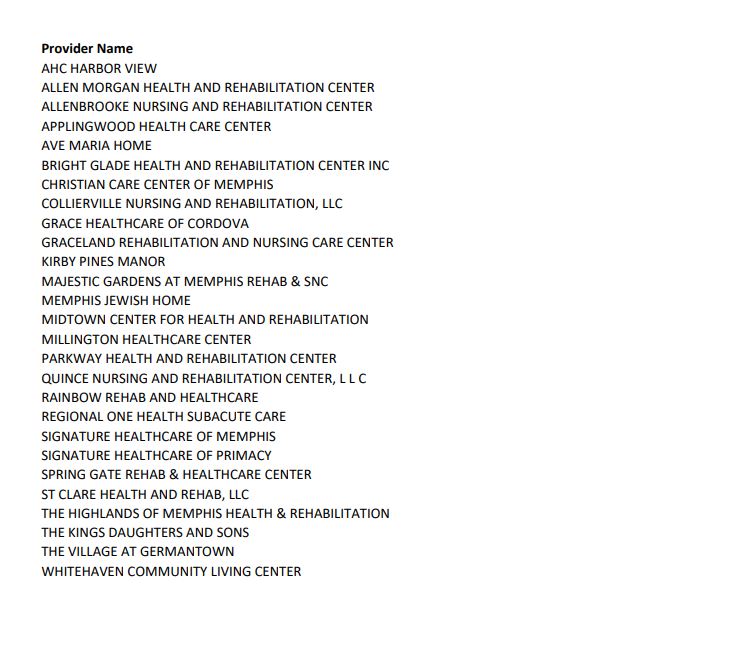
CMS sent tests to more than 700 nursing homes in Arkansas, Mississippi and Tennessee. WREG found more than 300 Tennessee facilities on the list, including 27 in Memphis. Below are the sites where testing kits were distributed.
The rapid tests save time and potentially lives. However, some claim, the type of testing offered by the federal government to be used on our most vulnerable population doesn’t provide enough protection.
“It’s like we’re inching toward it, but we’re not there,” said Brian Lee, a former government long-term care ombudsman, now running his own nonprofit watchdog called Families for Better Care.
“The tests that are in nursing homes now are just antigen based tests of the wrong kind of test. They only identify people who are symptomatic definitively if they have the virus or not,” he said.
Dr. David Aronoff, the Director of the Division of Infectious Diseases at Vanderbilt University Medical Center, explained the different types of testing to WREG.
“I think we have to be careful during a pandemic to make sure that we don’t let perfect be the enemy of good when we’re trying to save lives,” said Aronoff.
Testing falls into the follow categories:
- Molecular (sometimes called PCR)
- Antigen (sometimes referred to as rapid)
- Antibody
Molecular and antigen are diagnostic and testing for active infection. Antibody tests can reveal previous exposure.
“Right now, the gold standard test for infection is really the molecular test,” Dr. Aronoff said.
That’s because the tests are very sensitive, easily detecting small amounts of the virus, he said.
“They can detect very, very small levels of this genetic RNA material in our secretions. The good thing about them is that they’re very sensitive, so they’re likely to find very low levels of genetic material.”
Due to that sensitivity, however someone could test positive, but no longer be contagious.
“So, for example, after I recover from COVID-19 and I’m no longer contagious, I might be positive by molecular tests for many, many weeks beyond that,” Aronoff said.
The turnaround time on molecular tests can run anywhere from 24 hours to a week.
“The antigen tests have the advantage of being relatively inexpensive to make. They are also very rapid, sort of like a urine pregnancy test. They’re almost that quick and they can be done at what we call the point of care,” Aronoff said.
However, antigen tests aren’t nearly as sensitive as molecular tests, requiring more virus to be present for someone to test positive.
“If there’s a lot of doubt that that person is actually infected, it would be very helpful to have a molecular test to be able to be done to confirm that positive test,” he said.
For nursing homes using the tests, the Centers for Disease Control and Prevention recommends that negative POC antigen tests be considered presumptive.
In an email sent to WREG, a CMS spokesperson said, “Fighting this global pandemic requires an array of different technologies, including antigen testing. In areas of high prevalence or for patients with known risk factors, positive results from an antigen test can be considered confirmatory and used for diagnostic purposes. In areas of high prevalence, confirming negative results using an alternative form of testing is recommended.”
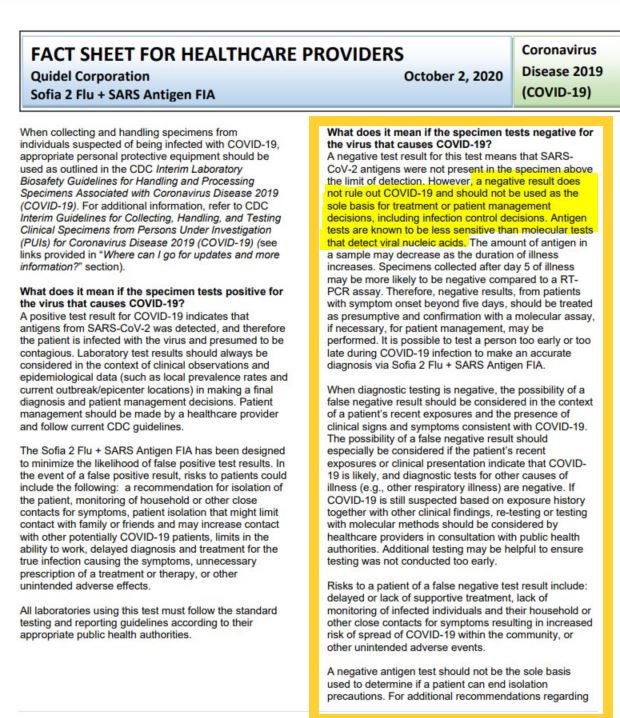
A fact sheet from one of the manufacturers also reads “a negative result does not rule out COVID-19 and should not be used as the sole basis for treatment.”
“They need to either read the fine print on the testing machines, the accuracy, the validity of the results, credibility, those results and get and really understand how they work and then get them the right machines and the right test,” said Lee. “We’re still seeing far too many of infections and far too many deaths in these nursing homes. And and innocent lives are being lost when we aren’t doing enough.”
Federal statistics show an increase in cases at nursing homes nationwide.
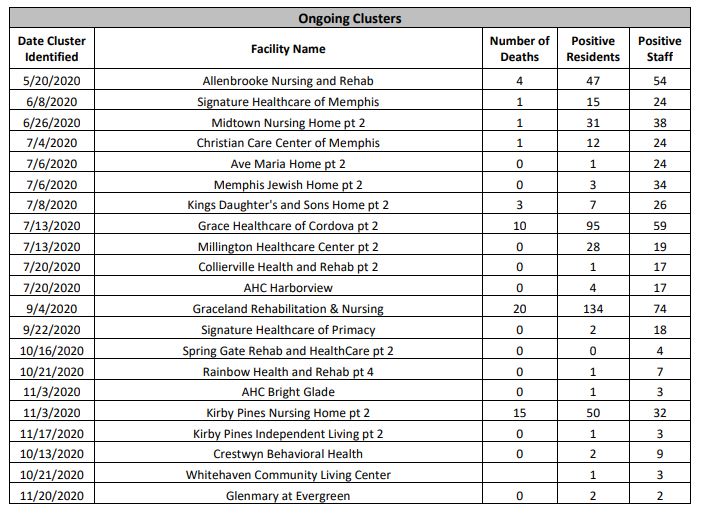
In Shelby County, there have been more than 50 outbreaks at long-term care facilities since the start of the pandemic.
Nearly 160 residents have died.
We’ve talked with relatives left behind, who questioned how the deaths happened, especially when visitation had been halted earlier in the year.
“What needs to be done to prevent this?” asked Sherryl Carlock.

Carlock’s aunt, Shirley Gatewood, lived 71 years with Down Syndrome but died of COVID-19. She was a resident at Graceland Rehabilitation and Nursing Center.
“Why are we consistently receiving more and more clusters? When no one is being allowed to go in except for staff,” questioned Carlock.
At Graceland, 20 people died (including a fatality added the week of Nov. 23), and 134 residents and 74 staffers have tested positive. The number of infected staffers at Graceland grew by a dozen in daily report issued by the Shelby County Health Department Tuesday, Nov. 24.
Out of the active clusters at facilities in Shelby County, nearly 500 staffers have been infected and it’s a number that’s increased lately.
Current federal guidelines require nursing homes test residents if they’re symptomatic, or if there’s an outbreak.
Staff testing depends on the county positivity rate, which was 11% for Shelby County for the week ending, Nov. 14.
Counties with a positivity rate greater than 10% are required to test workers twice a week.
David Sweat, Chief of Epidemiology with the Shelby County Health Department, explained how workers can unknowingly introduce the virus into an environment such as a nursing home.
“It’s very often the people who work there are actually the ones who come to the facility setting an organism. And then once it’s introduced into the facility, it spreads. But remember, with COVID-19, it is insidious because you will start shedding usually for two days. You will be shedding coronavirus prior to the onset of symptoms,” Sweat said.
“And this virus is three times more infectious than the flu. So it spreads more easily. But if a person is not showing signs or symptoms and they’re in between their tests, they can certainly be accidentally introducing virus into any environment.”
WREG asked, “So then how do facilities protect against that and then therefore help to better protect the residents?”
Sweat said everyone just does the best they can. “They exclude people who are ill. They exclude people with a positive test. They test frequently their staff to try to catch these things early, but, it’s very difficult.”
That is why Lee says the type of testing in an environment like a nursing home is even more critical to curb cases.
“Lives are too precious. We cannot get a loved one back once they have COVID and die from it. So it’s better now to get the right test in the nursing homes,” Lee said.
There are molecular, rapid tests on the market. In fact, there’s one that claims to deliver results in five minutes.
Aronoff said the pros of such tests are speed and high sensitivity of the test. The cons, however, are that they may be harder to access and more cost prohibitive for some.
The testing kits provided to nursing homes are a one-time shipment. We asked CMS about how fast they anticipated nursing homes would run out of tests, and how they were expected to pay afterwards.
A spokesperson said, “Nursing homes are responsible for ordering resupplies of tests/kits with the $5 billion in aid CMS has provided to them. After the initial shipment of instruments and tests, nursing homes will be responsible for procuring their own tests directly from the manufacturer or medical device distributor.”
Earlier this year, the state of Tennessee reimbursed nursing homes for testing. That funding stopped as of October 1, 2020.
WREG contacted several area nursing homes that received the rapid, point of care testing kits from CMS, but we haven’t received a response to our inquiries.